
The Hidden Layer in Your Point A: Endocrine Function
Introducing endocrine assessment into the Absolute framework of Point A.


We’ve built Point A around four pillars: Health History, Joint Assessment1, Treatment & Training History, Performance History.
Each one answers a version of the same question: where is this athlete right now, and how did they get here?
The Health History pillar—which we cover in depth in The Art & Science of Programming—captures energy patterns, sleep quality, body composition changes, stress load, and medications. All of it points toward the same underlying system that most coaches and clinicians never actually measure: the endocrine system.
It’s already in your Point A. But without objective data, it stays hidden—and historically, getting that data has been the barrier. Blood panels, salivary cortisol, urinalysis—these weren’t practical in most clinical or performance settings. So the endocrine picture remained a gap in the Point A profile.
It’s 2026. These are solvable problems.
And once we have that data, the question becomes the same one we ask everywhere else in the framework: is the endocrine system synced with the neurology, or has the neural network scaled past what the endocrine system can support? Because that gap—neurology outpacing endocrine function—is just as consequential as neurology outpacing connective tissue. It just takes longer to see, and it’s easier to miss without the lab work to prove it.
The Problem With Ignoring Hormones
Picture the athlete we see most often in this situation. Three to five years into a serious training program. Neural network developed to Point B. Strong, fast, reactive—on paper. Training hard, recovering poorly. Body composition shifting despite no change in nutrition. Sleep degrading. Performance outputs inconsistent in ways that don’t match the programming. And somewhere in the last six to twelve months, a soft tissue injury that didn’t make sense given the load they were under.
This is the athlete whose neurology got there first. The connective tissue couldn’t keep pace. And underneath both of those—quietly decoupling from the entire system—the endocrine environment that was supposed to be funding the adaptation.
The coaches and clinicians working with this athlete are usually looking at only the training log. But they need to also look at the lab work to get a complete Point A.
Here’s what we already know: the nervous system can outpace connective tissue. That gap—neurology ahead of biology—is where reactive strength injuries live. Achilles ruptures, hamstring tears, UCL blowups. The tissue can’t keep up with and express the force the neural network of absolute strength is generating.
What we haven’t talked about yet is that the nervous system can simultaneously outpace the endocrine system.
And when that happens, programming alone isn’t enough.
You can conjugate all four Point B elements perfectly. You can run the Bulgarian strategy for connective tissue at 21 sessions a week. You can have the most sophisticated training strategy. And if the athlete’s endocrine system is already in failure mode, you’re pushing against a wall.
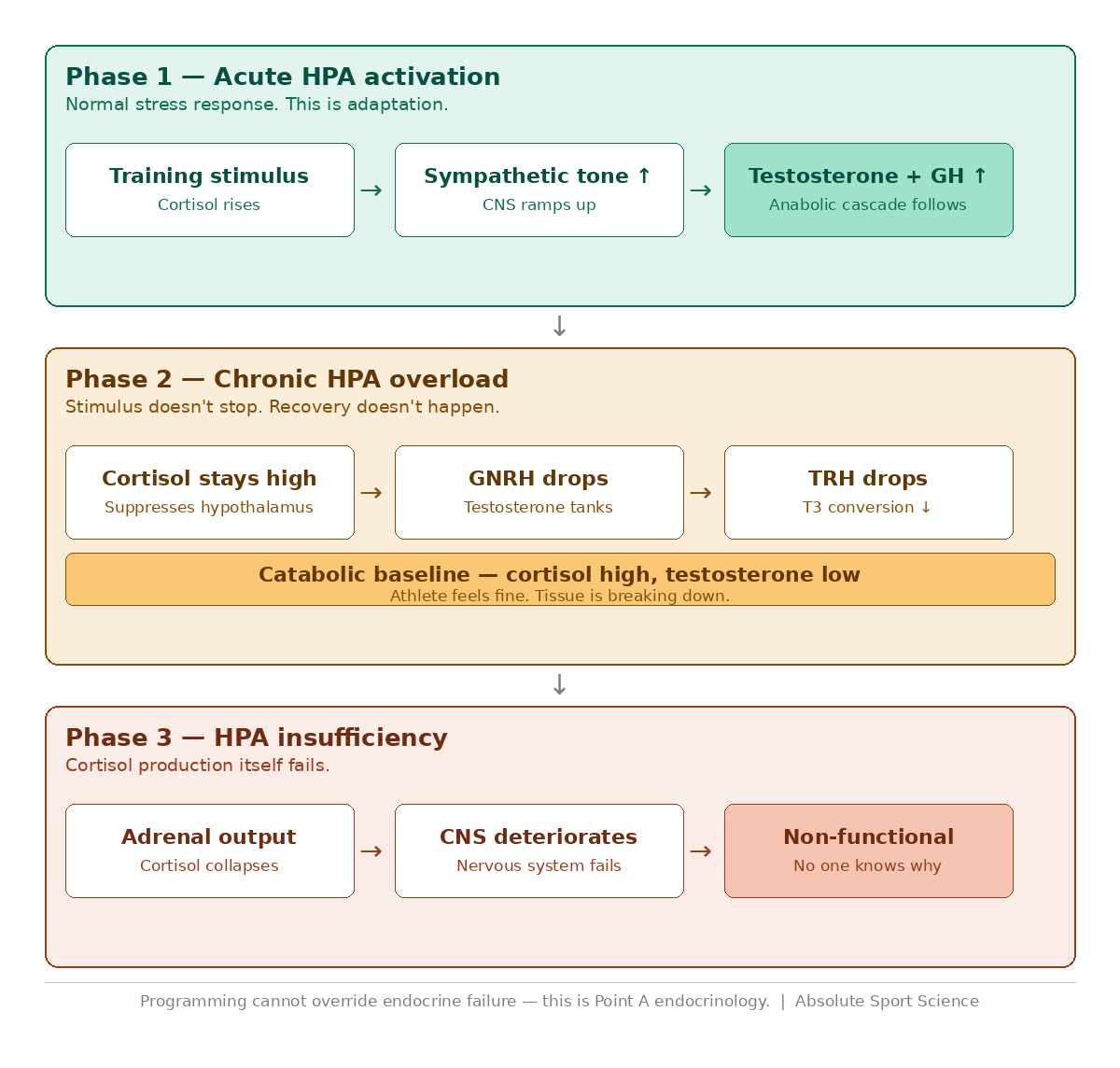
The Cascade
Phase 1 — Acute HPA Activation: A training stimulus hits. Cortisol rises. Sympathetic tone increases. Anabolic hormones—testosterone, growth hormone—follow in cascade. This is normal. This is adaptation.
Phase 2 — Chronic HPA Overload: The stimulus doesn’t stop, or the athlete doesn’t recover. Sustained cortisol suppresses the hypothalamus. GNRH drops, which tanks testosterone. Chronic HPA axis activation suppresses thyroid function through at least three converging pathways: central suppression of the HPT axis via cortisol and inflammatory cytokines reducing TRH/TSH output; direct inhibition of thyroid hormone synthesis; and—critically—downregulation of deiodinase enzyme activity that shifts peripheral conversion away from active T3 toward metabolically inert rT3. Cortisol is high. Testosterone is low. The athlete is catabolic at baseline—even when they feel fine.
Phase 3 — HPA Insufficiency: Cortisol production itself begins to fail. Nervous system function deteriorates. The athlete becomes non-functional—and often, no one knows why.
This isn’t theoretical. We’ve seen it in the lab work. Testosterone at the floor. CRP inflammatory markers 300% above normal. Adrenal profiles showing excessive cortisol output alongside complete anabolic collapse. Athletes who look like they’re training hard but whose tissue is breaking down faster than it’s being developed.
The tissue degradation timeline matches the endocrine failure timeline. That’s not a coincidence.
This is where it connects directly to the injury pattern we’ve been building the framework around. Achilles ruptures, hamstring tears, UCL blowups—we’ve framed all of these as reactive strength injuries. Neurology outpacing connective tissue. The neural network generating force that the bottom-up biological architecture can’t transmit.
What the endocrine picture adds is this: if cortisol is chronically elevated and testosterone is suppressed, tissue repair is already compromised at rest. The athlete isn’t just undertrained biologically—they’re actively breaking down faster than they’re rebuilding. Every training session added into that catabolic environment pushes the gap wider. The connective tissue was already behind the neurology. Now it’s falling further behind with every session, even when the programming looks right on paper.
The endocrine failure doesn’t cause the injury. It accelerates the timeline to it.
What Point A Endocrinology Looks Like
We’re not talking about full endocrinology practice. We’re talking about three targeted assessment pillars that give us actionable programming data.
1. HPA Axis (Adrenal Function) The most complex of the three. A single blood cortisol draw tells you almost nothing—cortisol fluctuates hourly. What you need is the full picture: cortisol awakening response, diurnal rhythm, total output, free cortisol, stored cortisone, clearance rates. The Dutch Plus test (combined urinalysis and salivary cortisol) is the current gold standard for this.
2. Gonadal Function (HPG Axis) Testosterone, estrogen, and the full hypothalamic-pituitary-gonadal loop. The mistake most practitioners make is looking only at testosterone. Low testosterone with low LH tells you something completely different than low testosterone with high LH—the first is a pituitary problem, the second is a testicular problem. You need the axis, not just the output.
3. Thyroid Function (HPT Axis) Thyroid drives mitochondrial biogenesis and cellular metabolism. Under chronic stress, the body downregulates thyroid output as a survival mechanism. Checking TSH alone misses this entirely — you need the full HPT axis evaluation.
Growth hormone and IGF-1 round out the picture, but are lower priority given the broad normal ranges, especially in developing athletes.
The Subjective Layer
Lab work doesn’t exist in isolation. Before we can interpret an endocrine profile, we need to know how the athlete got there. Several health history data points flag endocrine dysfunction before a single test is ordered:
Energy patterns in the first 60 minutes after waking
Night waking between 2–4 AM (a specific cortisol dysregulation signal)
Resting heart rate trends despite maintained training volume
Body composition changes — particularly muscle loss with concurrent fat gain
Subjective symptom timeline in the 1–3 months prior to injury
That last one matters for a reason that isn’t obvious: the first time you assess an athlete may not represent their baseline. If they’ve already been injured or overtrained by the time you see them, the lab values you’re looking at are downstream of a dysfunction that started weeks or months earlier. The health history is what lets you reconstruct the trajectory.
The Intervention Layer
The intervention layer for this is already in development. If you’ve been following the Founders Meetings, you’ve heard us talk about peptides—specifically BPC-157 and TB-500—in the context of connective tissue repair. What that conversation didn’t cover explicitly is the endocrine dimension. BPC-157’s neuroprotective properties and TB-500’s role in extracellular matrix organization aren’t just tissue repair tools. In a chronically catabolic athlete high cortisol, suppressed testosterone, tissue breaking down faster than it’s rebuilding—they’re part of the anabolic cascade that makes adaptation possible again.
We work directly with performance staffs across professional sport, so it's worth noting: both TB-500 and BPC-157 are currently banned under WADA guidelines—and enforced across the major leagues (MLB, NFL, and NBA). We'll let you draw your own conclusions about what it means when governing bodies move to ban recovery compounds. Our read is that the biology doesn't lie—and neither do the results.
This is why we don’t treat peptides as a standalone recovery intervention. In the context of the Absolute Conjugate Strategy, they sit inside the reactive strength programming layer—specifically on the biological side. You’re running the Bulgarian strategy for connective tissue at 21 sessions a week. You’re progressing through the isometric continuum. You’re building bottom-up CT architecture. The complete reactive strength peptide stack is what ensures the endocrine environment isn’t working against every one of those sessions. It’s not a shortcut. It’s the biological infrastructure that makes the programming actually land.
Point B
Which brings us back to the question we ask about every element of the system: what does Point B look like here?
For the endocrine system, Point B is simple to define and hard to achieve. It’s the state in which the endocrine cascade is synced with neurological output—testosterone, growth hormone, and cortisol operating in a pattern that supports the tissue repair cycle, not works against it. The neural network is scaling. The connective tissue architecture is being built. And the endocrine environment is providing the biological infrastructure that makes both of those adaptations stick.
When the endocrine system decouples from the neurology—cortisol chronically elevated, testosterone suppressed, thyroid downregulated—you don’t have a training problem. You have a system problem. And no amount of programming sophistication closes that gap without first identifying it in your Point A.
That’s what this series is about.
What’s Coming
This is the framework. The first layer.
Over the next several articles, we’re going to go deeper into each axis—how the HPA cascade actually unfolds, what gonadal dysfunction looks like across different athlete profiles, how thyroid function interacts with the tissue repair cycle, and how all of it connects back to the Point A → Point B roadmap.
If you’re a clinician or coach working with athletes who are training hard but not recovering, not adapting, or getting hurt at a rate that doesn’t match the programming—the endocrine layer is worth looking at.
This is the framework we’re building inside The Art & Science of Programming. If you’re not in the course yet, that’s where to start.
More to come.
We utilize Functional Range Assessment (FRA) for our joint assessment.