
Nabers Has Never Been at Reactive Strength Point B Since High School
What a Chronic Left Toe, a Non-Contact ACL Tear, and a Second Surgery Are Telling Us—From a Reactive Strength Paradigm



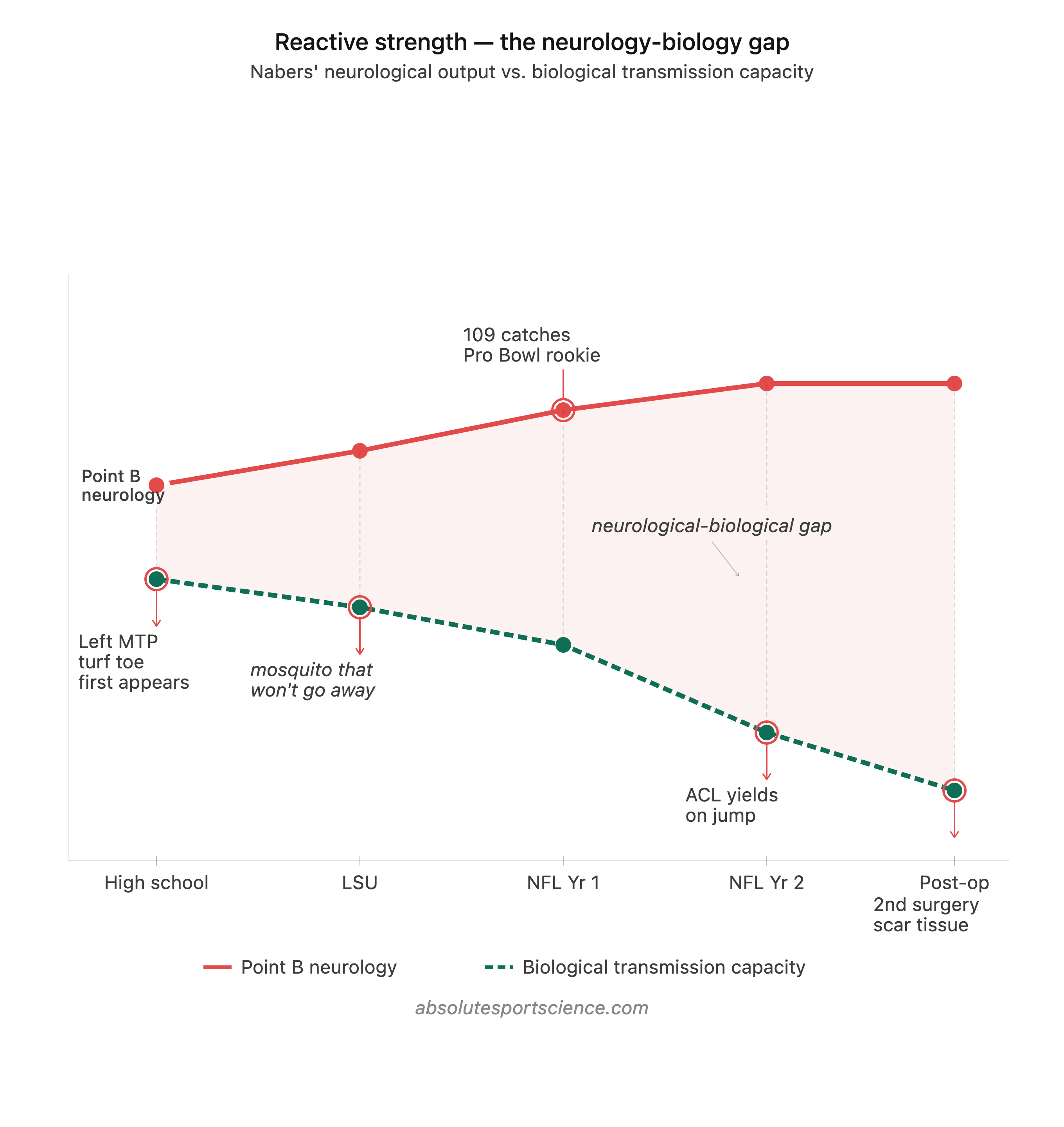
When a high-output athlete presents with a chronic soft tissue issue that won’t resolve—one that persists through daily treatment + training, and the full resources of a professional sports organization—the reactive strength paradigm asks a specific question:
Is the neurology outputting more than the biology can currently transmit?
Because if the answer is yes, the resolution is specific: you have to use the neurology to stimulate the biology. Deliberately conjugate specific treatment and training from a shared framework so that the neurological output becomes the stimulatory mechanism driving biological adaptation at the site of the deficit. Without that framework, the deficit doesn’t stay static. It deepens. What begins as a manageable soft tissue issue becomes chronic. What is chronic accumulates pathological change. And what accumulates pathological change eventually expresses itself as something that can no longer be managed—a structural failure at the point the system could no longer compensate through.
Malik Nabers has had a chronic left foot turf toe since before his college days at LSU. It followed him through two NFL seasons with the New York Giants. He called it “a mosquito he couldn’t kill”. The staffs around him worked on it continuously.
The mosquito never went away.
On September 28, 2025, Nabers jumped for a deep ball against the Los Angeles Chargers. His right knee gave way on the takeoff—not the landing. Torn ACL + torn meniscus. Season over.
That distinction matters. The tissue didn’t fail under the load of landing like Odell Beckham Jr.’s ACL rupture with the Cleveland Browns. It failed under the neurological output of the jump itself—the precise moment the nervous system fired maximally to generate force, and the biology couldn’t transmit it. That is not a contact injury or a landing mechanics problem. That is a reactive strength failure in its clearest form.
From a reactive strength paradigm, what happened to Nabers is entirely legible—and it was observable long before that moment. His injury record is a coherent clinical picture of what happens when elite neurological output runs ahead of its biological infrastructure for long enough, without a programming strategy in place to close the gap.
Naber’s Has Never Been at Biological Point B
When Nabers tore his ACL, sources noted that for the first time since high school, he would have a chance to be fully healthy.
At Absolute Sport Science, Point B describes an athlete’s full neurological and biological expression of all four physical capacities—operating concurrently and without inhibition. Absolute Strength is the maximal force the neuromuscular system can voluntarily produce. Speed Strength is the ability to express that force rapidly—at the highest attainable speed. Reactive Strength is the capacity to absorb, store, release, and dampen elastic connective tissue energy in conjugation with the neural network of absolute strength. And Joint Function is the range and neurological control available at each articulation to support all three. When all four are expressed simultaneously, the athlete is at Point B. Nabers has never occupied it.
From a reactive strength paradigm, this tells us his neurological output was already exceeding his biological tissue’s transmission capacity in his teenage years. That is not a weakness—it is the signature of an exceptional athlete. But it is also a programmable signal. A leading indicator visible early enough that a specific intervention strategy could have been built around it. That neurological output, channeled through a conjugated treatment and training framework, was the exact stimulus needed to drive biological adaptation at the site of the deficit.
Instead it ran unchecked. And the biology has been falling further behind ever since.
Reading Naber’s Through Point A
At Absolute Sport Science, every athlete assessment begins at Point A—the current state of the athlete across four domains: Health History, Treatment and Training History, History at Level of Competition, and Functional Range Assessment. Point A is what tells you where the neurology-biology relationship actually stands before you build a single rep of programming around it.
We don’t have access to Nabers’ full Point A. But the public record gives us enough to construct a partial picture—and that partial picture is, on its own, deeply informative.
Health History (available) Chronic left first MTP turf toe present since high school. Reported as never fully healthy since before LSU. Right knee ACL and full meniscus repair October 2025. Arthroscopic debridement of scar tissue, right knee, spring 2026. Two surgical procedures on the same joint within eight months.
Treatment and Training History (inferrable, not confirmed) Continuous daily treatment across LSU athletic training staff and two years with the New York Giants medical and performance staff. Pre-hab protocol implemented prior to October surgery. Elite training environment throughout. Specifics of modalities, loading strategy, and programming philosophy are not publicly available—but the outcome of those years of work is clear: the turf toe never resolved. From a reactive strength paradigm, that outcome tells us the strategy—however well executed in isolation—was not conjugated around a shared model with a mechanism for resolving a reactive strength deficit at its root. Treatment addressed the biology. Training built around it. But neither, operating on separate tracks, had a framework for using the neurological output to drive biological change at the site.
— Reactive strength assessment: the missing methodology Assessing reactive strength means overlaying two systems. The first is neurological output (top-down element)—measurable through RSI protocols and force plates, technology every NFL team has access to. That half is commoditized. The second is a tissue-based assessment (bottom-up element) of the length-tension curve of the connective tissue at the site of the deficit—and this half cannot be outsourced to a machine. It requires a trained human practitioner with cultivated clinical skill and the knowledge framework to interpret findings in the context of the neurology-biology relationship. Overlaying both makes the gap visible as a number, not just a clinical impression.
That practitioner skill is the bottleneck. It’s not a technology problem. The tissue-based half requires human intelligence that has to be deliberately developed—and it is the core of what we apply in the reactive strength module inside The Art and Science of Programming. Applied to Nabers, this overlay at the left first MTP at any point in his career would have shown exactly how wide the gap was—and whether the interventions were closing it.
History at Level of Competition (strong) LSU starter. NFL rookie record 109 receptions. Pro Bowl Year 1. Elite route precision and first-step quickness documented extensively at every level. Missed OTAs and training camp reps across both NFL seasons due to the left foot. Exited four games into his sophomore year with the ACL injury. Performance at full expression has never been sustained across a full season of professional football.
Functional Range Assessment—Joint-by-Joint Movement Capacity (unavailable) The FRA quantifies the joint function component of Point B—distinguishing between passive range, active range, and the degree of neurological control the athlete can express within that range at each individual articulation. That distinction identifies whether the deficit at a given joint is biological, neurological, or both, and therefore which system is the rate limiter. In addition, the CARs analysis from FRA helps us quantify the amount of movement that occurs externally at each articulation to allow for the observation of areas of movement that may be deficient or inadequate. An FRA of the left first MTP, left ankle, and right knee would have provided the joint-by-joint map the reactive strength assessment overlay sits on top of. Without it, the work was being done without a map.
The Mosquito Was the Signal
Turf toe is, at its core, a reactive strength injury. The first MTP joint is the final transmission point in the lower extremity force output propulsion chain—every route, every cut, every takeoff passes through it. When it is compromised, the nervous system doesn’t reduce its output. It neurologically shields around it, shifts load, and reorganizes movement to protect the site.
For Nabers, that shielding has been active since high school—on the left side. Every rep executing with a neuromuscular system already protecting the left forefoot by asking more of the right lower extremity. Every season, the left-right asymmetry deepened. Every season, the probability climbed that the right side would encounter a demand it could not meet.
The right knee ACL was not random. It was the endpoint of a compensation chain building, compounding, since before he was recruited to go to LSU, let alone drafted in the NFL.
The resolution was always available. That same neurological output driving the compensation was the stimulus that could have built the biological foundation the left foot needed—through a conjugated treatment and training strategy designed to use it that way. That is what treating reactive strength means. And it is what years of managing pain and symptoms of the toe, without that special strength capacity framework, could not provide.
Michael Thomas: What Elite WR Output Actually Looks Like
To understand the magnitude of force the neural network of an elite wide receiver generates—and what the reactive strength of the foot and ankle must be capable of transmitting—consider what happened to Michael Thomas.
Thomas is not just any receiver. In 2019 he was named NFL Offensive Player of the Year—the best offensive player in the entire league, not just at his position—after catching 149 passes in a single season, the NFL single-season reception record. That designation is Point A information. It tells us the neurological output Thomas was operating at—the force his nervous system was generating through every route, every cut, every plant and release—was at the absolute ceiling of what the human performance system produces at the professional level.
In Week 1 of 2020, a defender was thrown onto his left ankle, tearing the deltoid ligament and surrounding structures. Two years of recovery followed. When he returned in 2022, three games in, he left the field against the Panthers with a toe injury. No contact recorded.
The diagnosis: a dislocated second toe on his right foot.
Not a sprain. A dislocation—the joint forced entirely out of position by his own neuromuscular output. Nothing external caused it. The neural network fired at the level it always fires at elite output. The foot and ankle, which must have sufficient reactive strength to receive and transmit that force, could not. The joint gave way.
This is the reference point for what the reactive strength of the foot and ankle is required to handle at the elite wide receiver level. The force being generated is so significant that when the biological capacity to transmit it is compromised—through injury, asymmetry, or accumulated deficit—the tissue doesn’t just strain. It blows up and dislocates the joint.
The neurology outputs violence onto the tissues at these levels of elite output.
Now consider that Nabers was showing connective tissue issues at the foot since high school—before the professional workload, before NFL-level speeds, at a lower cumulative load and with less provocation. His neurology is operating at that same elite output ceiling. The reactive strength demand on his left first MTP has always been at that level. And the biology has never been built to fully meet it.
Absolute’s Prediction for Naber’s in 2026
The conversation will center on timing. Week 1 or not. Same player or diminished. From a reactive strength paradigm, we can be more specific than that.
Nabers will return in 2026 carrying more biological limitation than he has ever had—on both sides of the lower extremity simultaneously. The right knee is post-surgical twice over, with connective tissue architecture still organizing. The left foot deficit that started this entire cascade remains unresolved. As of mid-June 2026, he is reported to be over 70% through his rehab and targeting Week 1—but from a reactive strength paradigm, a return timeline is not a resolution. His neurological output will return to elite levels faster than his biology can meet it—because that is exactly what it has always done. That gap has been widening since high school. Two procedures on the right knee have added variables to that side that weren’t there before.
What that looks like on the field: flashes of the exceptional neurology that made him a Pro Bowl receiver as a rookie, constrained by a biological system on both sides that cannot yet fully transmit what the nervous system is asking of it. Route precision will return before top-end reactive strength. First-step neurological quickness will return before the ability to sustain it across a full game at full output. The early weeks of his return will look like Nabers—and they will also look like an athlete whose biology is still catching up to his neurology.
This is not a prediction about his character, his work ethic, or his will to compete. Those have never been in question. This is a prediction about the neurology-biology relationship that the reactive strength paradigm makes visible—and what it tells us will happen when an athlete with Nabers’ output profile returns to full-speed football before both sides of his lower extremity have been built to meet that output through a conjugated programming strategy designed to close the gap at the root.
The question for 2026 isn’t whether Nabers comes back.
It’s whether the strategy around him is finally built to close the gap that has been widening since high school.
The remainder of this article—covering our clinical read of the ACL mechanism from the video and injury record, what the second surgical procedure tells us about the post-surgical reactive strength deficit now present on the right side, and the three-component programming strategy the reactive strength paradigm demands for an athlete with Nabers’ profile—is available to paid subscribers.
If the reactive strength paradigm is new to you, the learning module is the right place to start:
The Art & Science of Programming—Absolute Sport Science →
When the ACL Yielded—What Was Happening at the Knee
